The drugs we tested on SSS
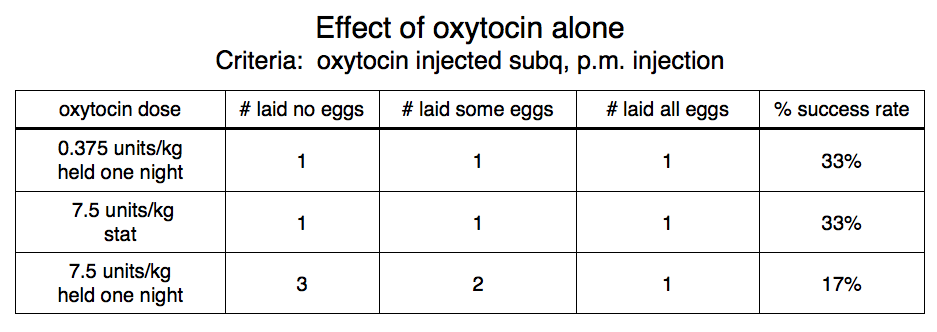
Although we doubted oxytocin used alone would be very effective on SSS we tried it at two dosage levels, after different holding periods, with a low success rate in all cases, as shown below.
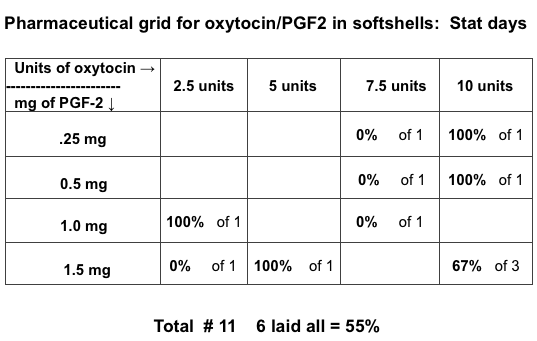
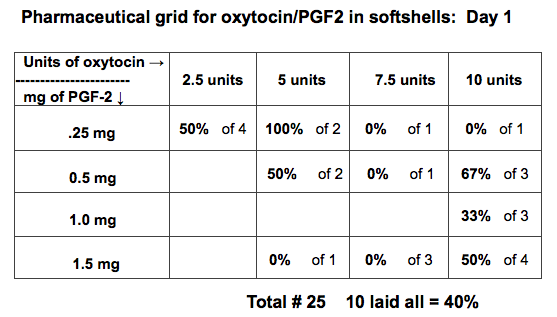
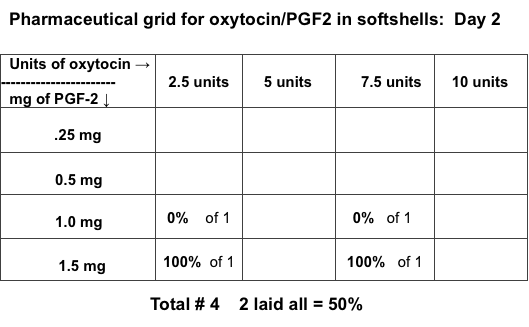
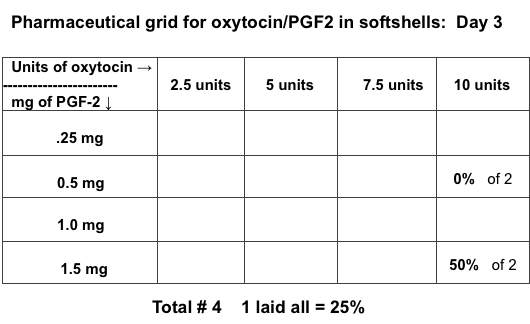
After trying oxytocin alone we ran a trial of a mix of oxytocin and Lutalyse with both drugs being injected at the same time. Forty four animals were involved. It took nine working to collect and process this many animals so numbers were low in every category. As you can see from the four tables below the success rate seemed higher on the stat day than on days 1, 2, 3 and 4.
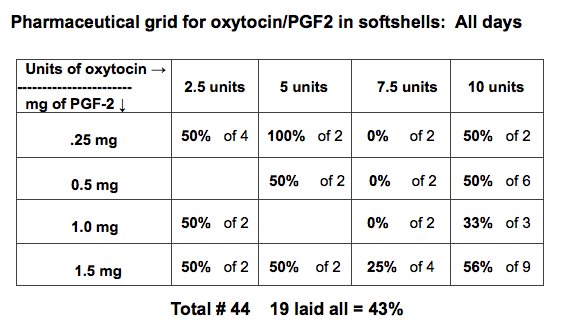
Even when all the results were pooled without specifying the day of induction, as shown below, none of the combinations of oxytocin and Lutalyse were very effective.
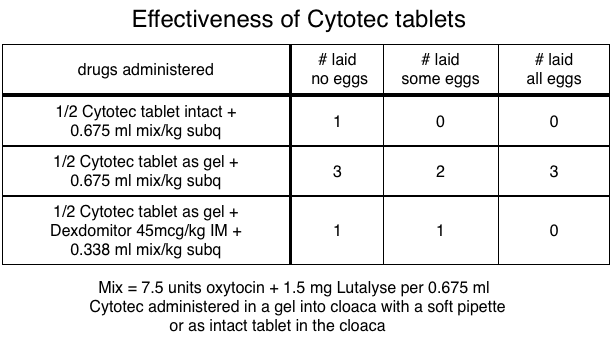
Cytotec is misoprotol or prostaglandin E1. This is a drug that can induce abortion in mammals. The details of how we used it are described previously under the heading “The drugs we used on their own.” The table below illustrates that it was not very effective. It was also time consuming to prepare and dangerous to instill so we abandoned its use.
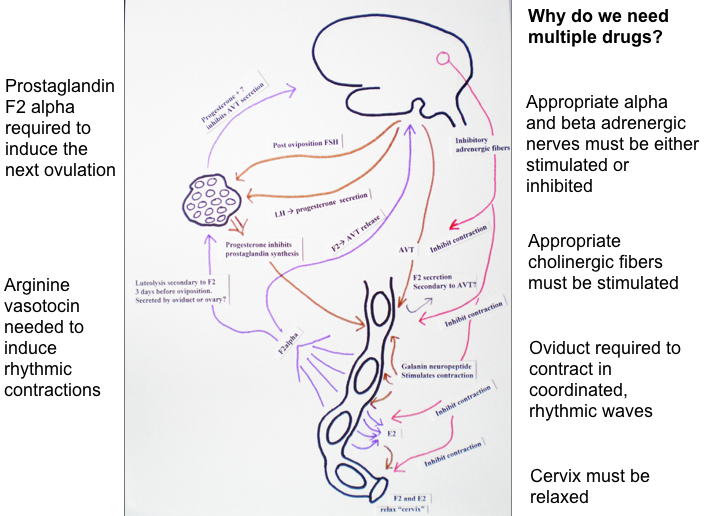
Propranolol is a beta-blocker. This class of drugs blocks the beta-adrenergic effects of peripheral nerves as shown by the red lines in the drawing below. It is the action of these adrenergic nerves that inhibits the oviductal smooth muscles and enables a turtle to stop laying eggs when it is disturbed (Gross et al. 1992). It has been found that propranolol can help stimulate oviposition in some lizards (Jones 1982) and birth in humans (Sanchez-Ramos 1996). We thought it might also help prevent a turtle from inhibiting oviposition induced by Lutalyse.
Before starting to work with propranolol we had to determine what a safe dosage was. To do that we hooked up several RES to an EKG machine and determined the minimal dosage that slowed the heart rate.
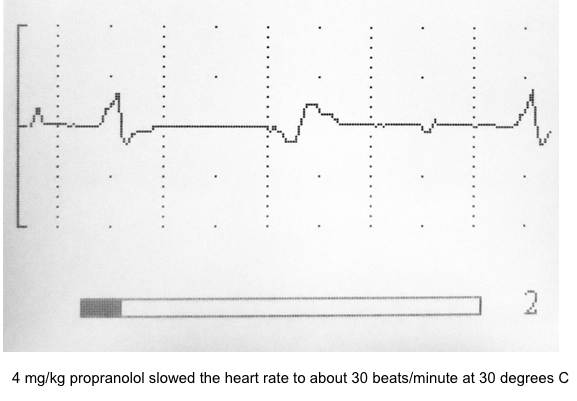
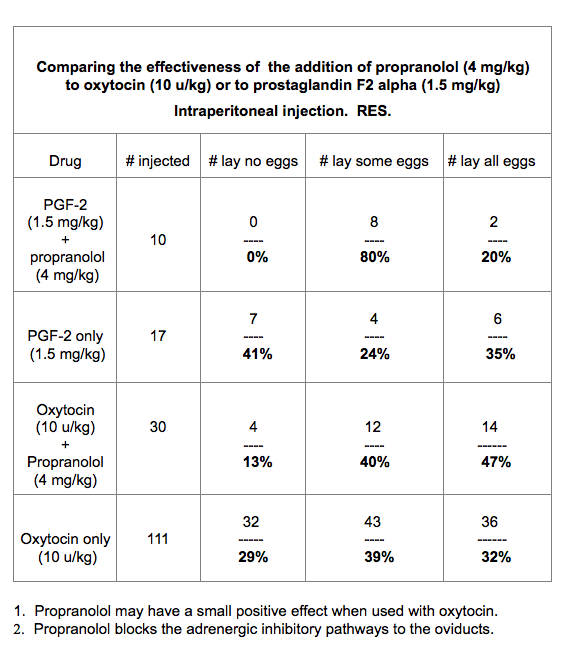
The minimal dose of propranolol that slowed the heart rate was 4mg/kg; the same dosage that Cipolle et al. found effective in 1986. This is a much higher dosage than is used in mammals. This introduced a new complication. Injectable formulations of propranolol for human use are too dilute for turtles. That meant we had to purchase the powder and mix it ourselves which made it impracticable for general applications. We first tried propranolol with RES in 2009 when we were still injecting intraperitoneally. The results are shown in the table below. As you can see the outcome was disappointing. Even Lutalyse, when used alone, had only a poor 35% success rate when injected into the peritoneum of RES. When injected subq in RES the success rate with Lutalyse was 94%!
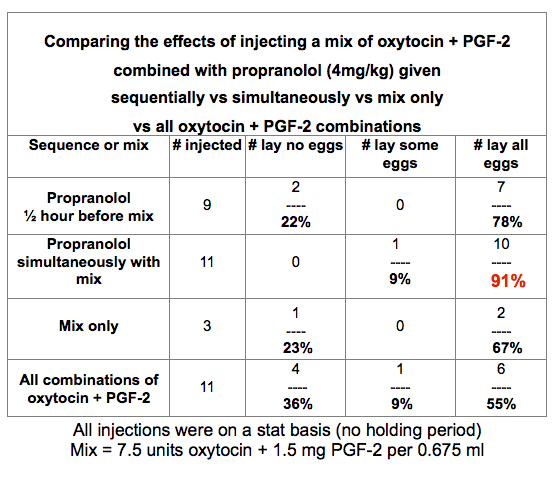
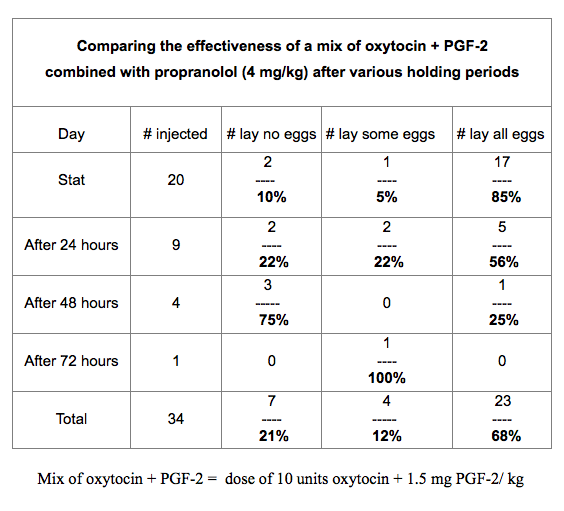
Our first trials in 2010 with propranolol in SSS produced a dramatic response. When we gave propranolol at the same time as a mix of oxytocin (20.0 u/ml) and Lutalyse (5.0 mg/ml) several hours after the SSS were captured we had a 91% success rate. However, when we ran a trial the same year with SSS held for various holding periods the success rate dropped rapidly the longer we held the animals before inducing them. These two tables are shown below.
In 2013 we tried to duplicate those results for a third time when we gave the propranolol 20 minutes before the Lutalyse after various holding times. The results are shown below; they were not nearly as successful as giving the drugs simultaneously in 2010.
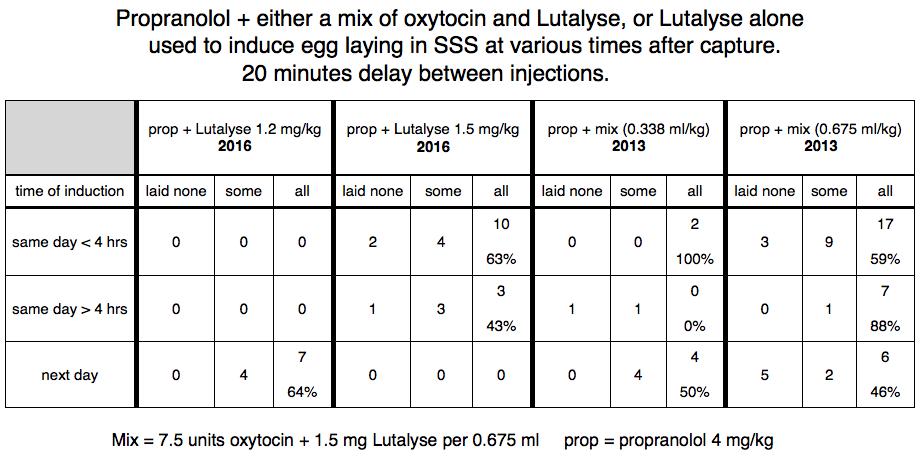
In 2016 we ran some more trials combining Lutalyse with propranolol (also shown in the chart above). We were unable to duplicate the excellent results we got using oxytocin+Lutalyse+propranolol in 2010. It was not clear to us if the problem was we didn’t add oxytocin to the mix or the propranolol solution was somehow altered. This was a real possibility because in 2016 we ordered the propranolol from a compounding pharmacy and did not mix it ourselves. Never-the-less, we abandoned the use of propranolol because it was not practical outside a lab.
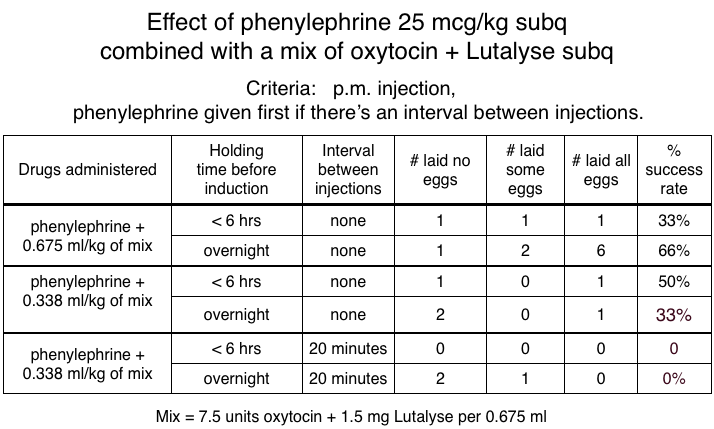
Phenylephrine is a selective alpha-1 adrenergic receptor activator. We thought it might have a positive effect on oviductal contraction (Gross et al. 1992), thus potentiating the egg laying process. As you can see from the table below, it did not work.
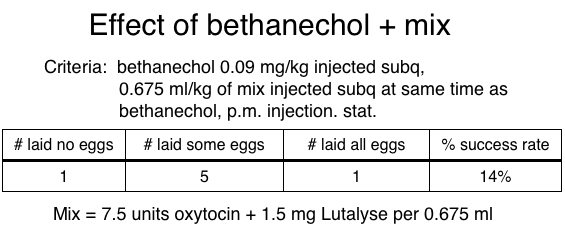
Bethanechol is a parasympathomimetic that selectively stimulates muscarinic receptors. We also thought this might enhance oviductal contractions. The table below shows it did not. What is interesting here is that both phenylephrine and bethanechol had a positive effect on the success rate with RES but had no such action with SSS; another illustration of the differences in the neurological systems of different species of turtles.
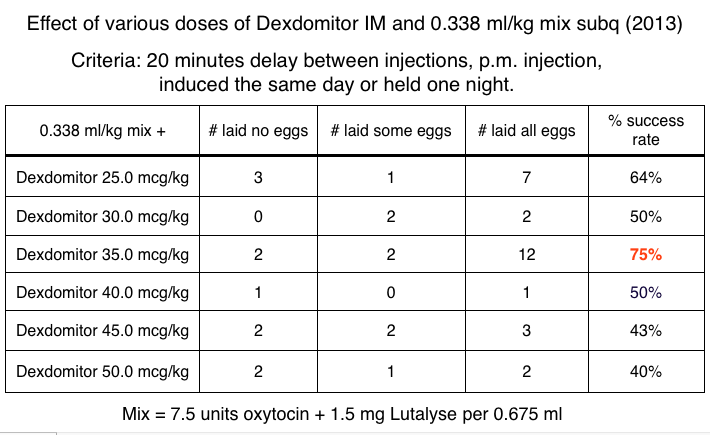
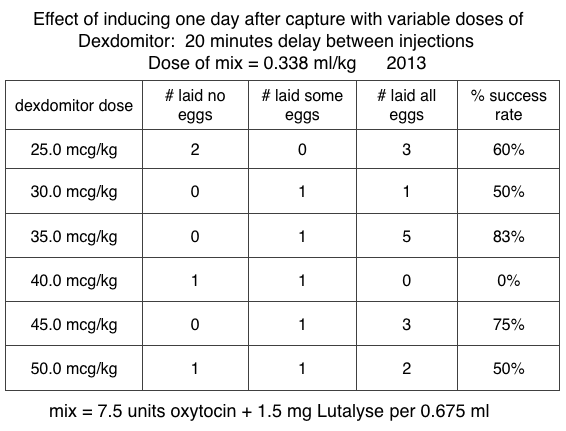
In 2013 we began to experiment with alpha-2 agonists in SSS. At the time we used Dexdomitor, an easily available agent used frequently by veterinarians. We injected it 20 minutes before the mix of oxytocin and Lutalyse. As you can see from the table below, it had a strongly positive effect, even when the dose of Lutalyse was only 0.75 mg/kg.
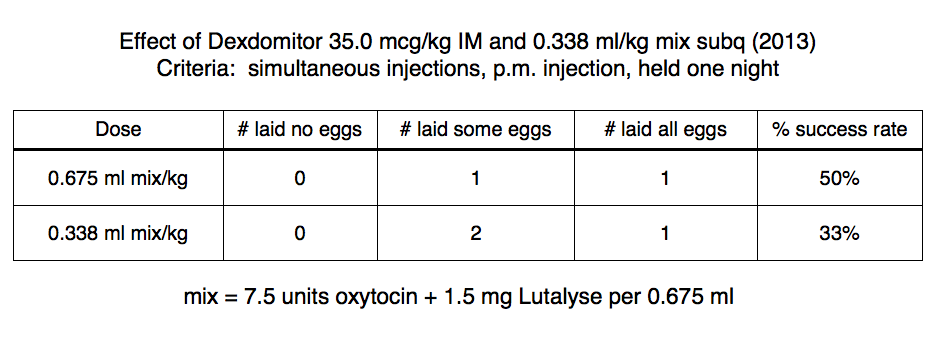
The chart below shows that when we repeated the procedure giving the drugs simultaneously the success rate dropped sharply.
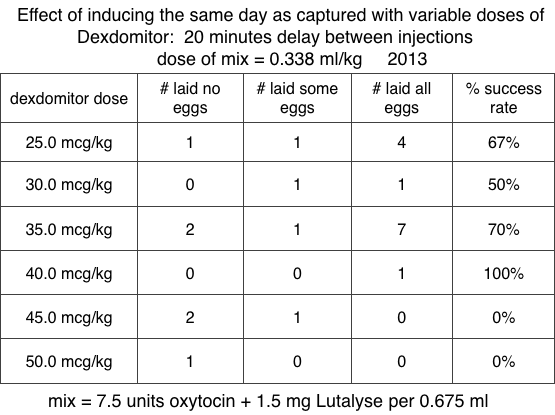
As you can see from the two tables below, we then divided the SSS into turtles induced with Dexdomitor on the day of capture and animals induced the next day. Unlike the results with propranolol, the success rate was about the same on both days. This meant there are two advantages to using an alpha-2 agonist over propranolol: the drug is easily obtained and works equally well on either of the two days after capture.
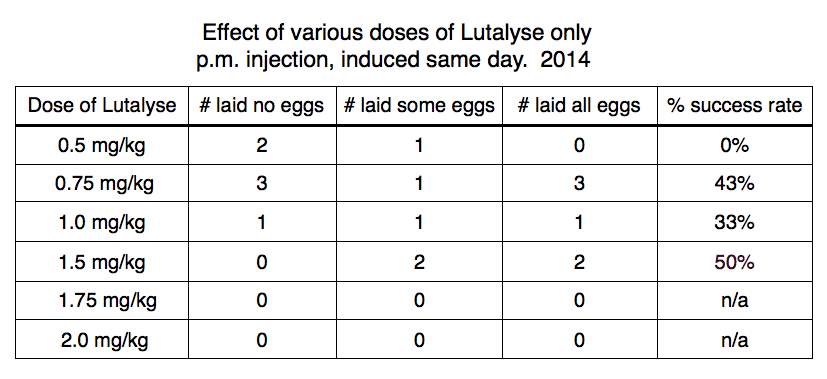
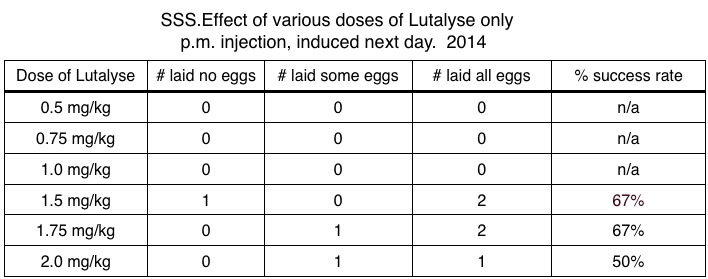
By 2014 we had realized that Lutalyse was the active ingredient in the combination of oxytocin and Lutalyse. We tried using Lutalyse alone in various doses with the SSS. The two tables below divide the SSS into turtles induced either the same day as captured or one day after capture. Lutalyse alone was as effective as the various combinations of oxytocin and Lutalyse had been but the success rate was clearly inferior to when an alpha-2 agonist was added.
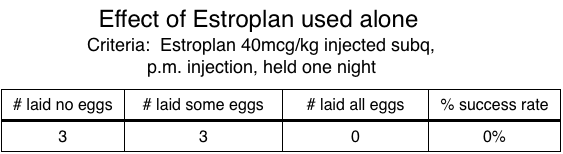
Estroplan (cloprostenol sodium) is another synthetic analogue of prostaglandin F2-alpha. Though it was not successful with RES we reasoned it might be effective with SSS. The table below shows that it wasn’t.
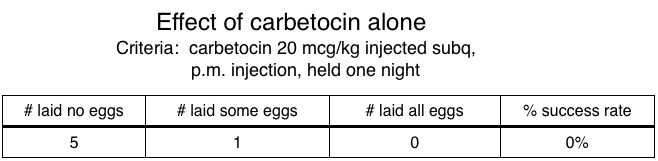
We also tried carbetocin, a synthetic analogue of oxytocin. It had failed with RES and also failed with SSS, as shown below.
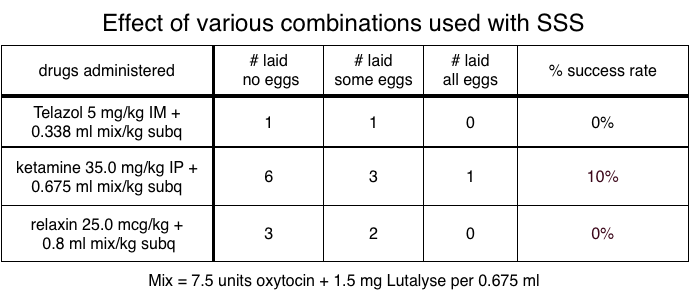
Attempts using relaxin, Telazol and ketamine in small numbers of SSS were also unsuccessful. Those results are shown below.
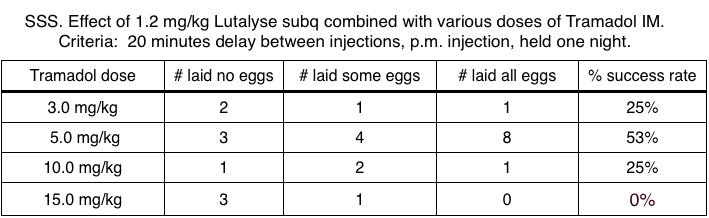
Tramadol, an analgesic used in mammals, increases the amplitude and duration of uterine contractions in some pregnant animals (Yakovleva 2017). Unfortunately, the chart below shows it had no such effect in SSS. Instead it made the animals agitated for 1-2 hours!
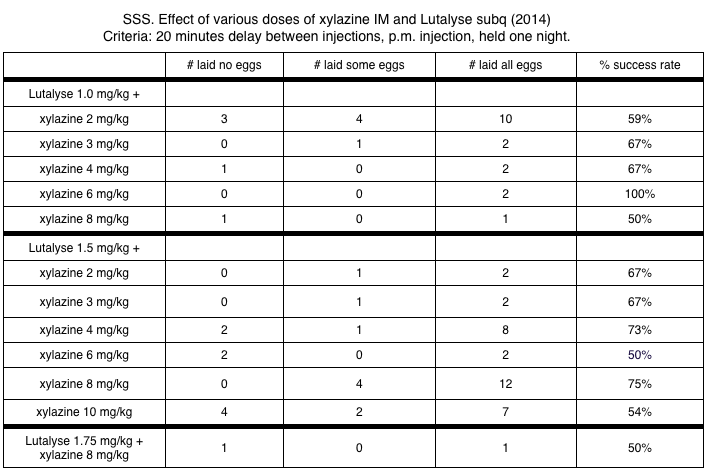
Xylazine is the second alpha-2 agonist we tried. Like Dexdomitor, it increased the success rate significantly when compared to using Lutalyse alone. This trial suffers from low numbers because there were so many categories. We had to capture about 90 turtles over 22 days just to process those categories.When we noted a drug combination that was initially successful we did more trials of that combination. The table below shows the best success rate was with xylazine 4-8 mg/kg combined with Lutalyse 1.5 mg/kg.
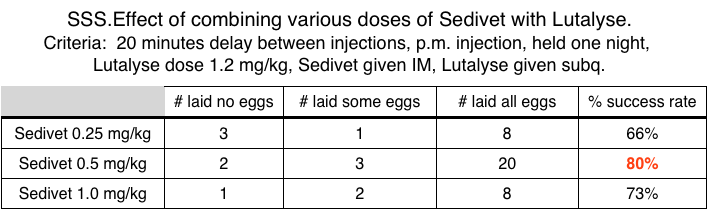
Sedivet is another alpha-2 agonist that is used in mammals. Based on our trial results with Dexdomitor and xylazine, and the standard doses for Dexdomitor and xylazine in horses (which vary widely), the expected best dose of Sedivet for SSS is between 0.175-0.4 mg/kg. The same comparison process with dogs yields an expected dose of Sedivet of 0.23-0.53 mg/kg for SSS. For this reason we experimented with Sedivet dosages between 0.25-1.0 mg/kg IM.
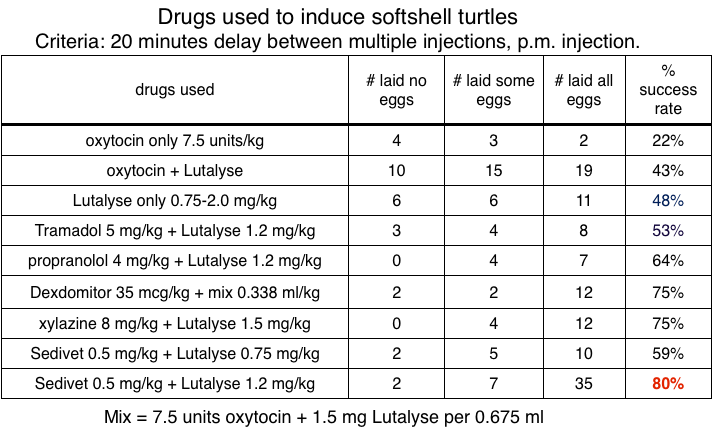
The table below shows the result of trials of different doses of Sedivet. The most effective dosage was 0.5mg/kg when combined with Lutalyse 1.2 mg/kg. We selected a Lutalyse dosage of 1.2 mg/kg because that seemed most effective in some of the propranolol trials.
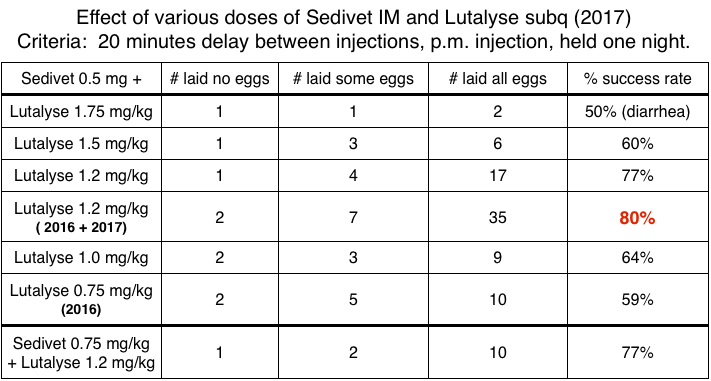
The results in the table below confirmed 1.2 mg/kg as the best dosage of Lutalyse when combined with 0.5 mg/kg of Sedivet.
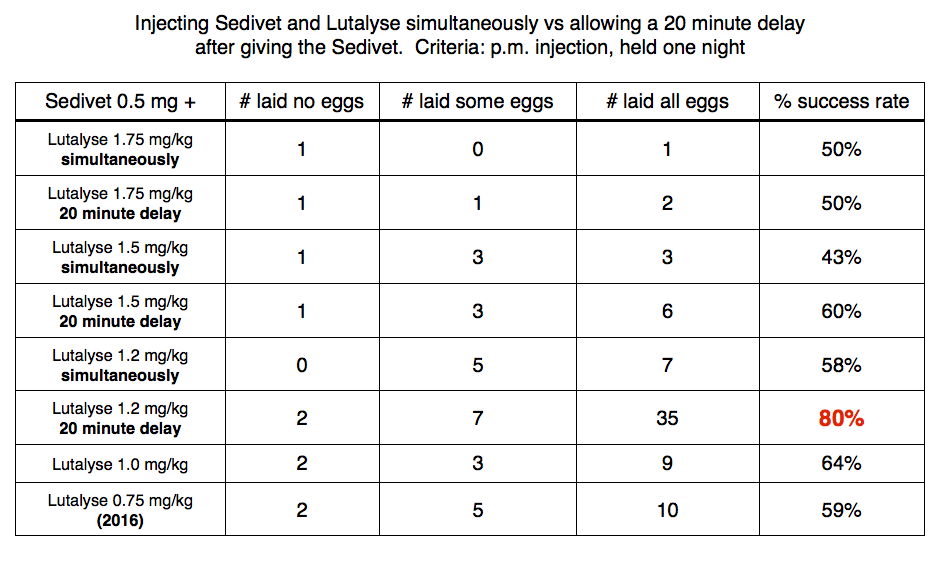
We then wondered if it was really necessary to wait 20 minutes between the Sedivet and the Lutalyse. The results below confirms that the 20 minute wait is necessary.
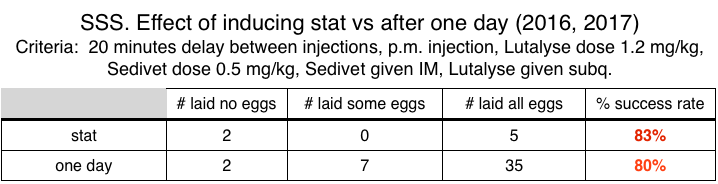
The next criteria we wanted to check is if it mattered if we induced the animals on the day they were captured or the next day. The table below shows it did not seem to matter when they were induced. This is in agreement with the results that we got using Dexdomitor.
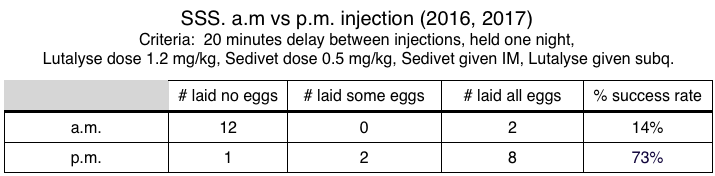
Then we wanted to know if we got better results if we induced in the morning or evening. Inducing in the morning meant we had to stay out of the lab the rest of the day to avoid disturbing the turtles. Fortunately, the table below shows the success rate was higher in the evenings.
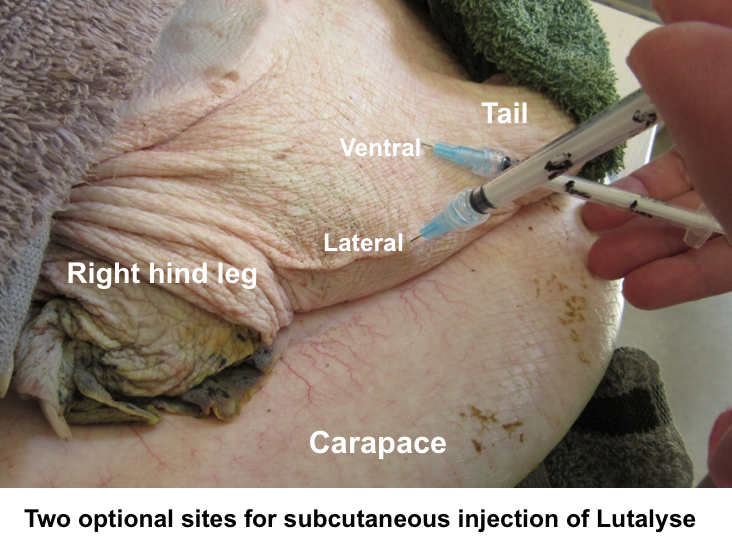
Finally we wanted to check if the site of the subcutaneous injection had any significance. The sites we tried are shown below.
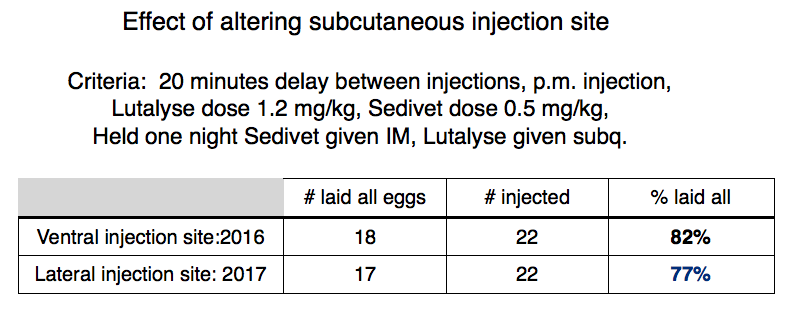
The table below shows the subq site did not matter.
A summary of all these results with SSS is shown in the table below where the success rate with Lutalyse plus Sedivet was followed closely by the success rate with Dexdomitor or xylazine plus Lutalyse.